
Episode 59
The BIG Announcement: ResiLearn

Educators in Medicine,
In this newsletter, we continue our journey through the fundamentals of AI, its applications in medicine, and its transformative role in faculty development and education. Let’s dive in.
Last week I had an absolute blast at AAFP Residency Leadership Summit. I met many old friends, and made many new ones. This is where I made the largest stage announcement that I mentioned last episode. If you’re new here, we’re glad to have you!
Okay. I need to confess. This episode isn’t a conference recap.
This is the story of a problem I experienced, a breaking point, and the accidental platform that came out of it.
This is the story of ResiLearn.
The Honest Truth About Being a New Program Director
When I became a Program Director, I assumed the hardest part would be teaching clinical complexity, the ACGME paperwork, or the institutional policies.
What has actually kept me up at night? I don’t know how my residents were really doing.
Picture this hypothetical: A resident is eight months into their second year. Clinically, they seem fine. Attendings aren’t raising concerns. They show up, they’re pleasant, they document reasonably well. And then the In-Training Exam scores arrive — and they’re in the bottom quartile, more than half way through their training.
The program director is sitting there thinking: How did I not see this coming? We paid for the board review course…
My answer: the program director didn’t have the data. And honestly? Nobody did. We want to build up competent clinicians based on delayed evaluations, and a once-a-year high-stakes exam. That is not a system.
The “Black Box” Problem
In GME competency assessments are scattered across spreadsheets, EPAs, milestone forms, and whatever your program coordinator is heroically tracking in the color-coded excel documents. We pay for expensive third-party QBanks, but the data stays trapped inside them — you can study from them, but you can’t use that performance data to actually run your program, design curriculum, etc. Residents binge-study before the ITE like it’s a Netflix series, and program directors only find out knowledge gaps when things are already an issue.
The kicker? We have the tools to do better. Speaking directly for Family Medicine programs for now: we have ABFM practice content. We have milestone/CBME frameworks. We have decades of learning science on spaced repetition and retrieval practice. We have gamification research. We just weren’t connecting any of it.
So I decided to do something about it.
Fix it Mode.
My programming background started with the quadratic formula on my TI-83, and the HTML I used to build my middle school webpage. It had a spinning earth and a starry sky background. I was very proud. I did learn python later but not much.
But here’s what I’ve been writing about in this newsletter for months: the time we’re in has fundamentally changed what people like us — clinicians, educators, people who spot problems — can actually build. Using AI tools, I started constructing what would become ResiLearn.
My wife (who has immense patience) can confirm this happened during many hours I should have been sleeping. But, what started as a personal fix for my own program slowly grew into something I learned (through many conversations) other program directors needed just as badly. So here we are.
What Is ResiLearn, Actually?
ResiLearn is a gamified, competency-based learning platform built specifically for graduate medical education. Think of it as what happens when a QBank decides to actually help PDs instead of just grading residents silently.
🎮 For Residents: Make Studying a Habit
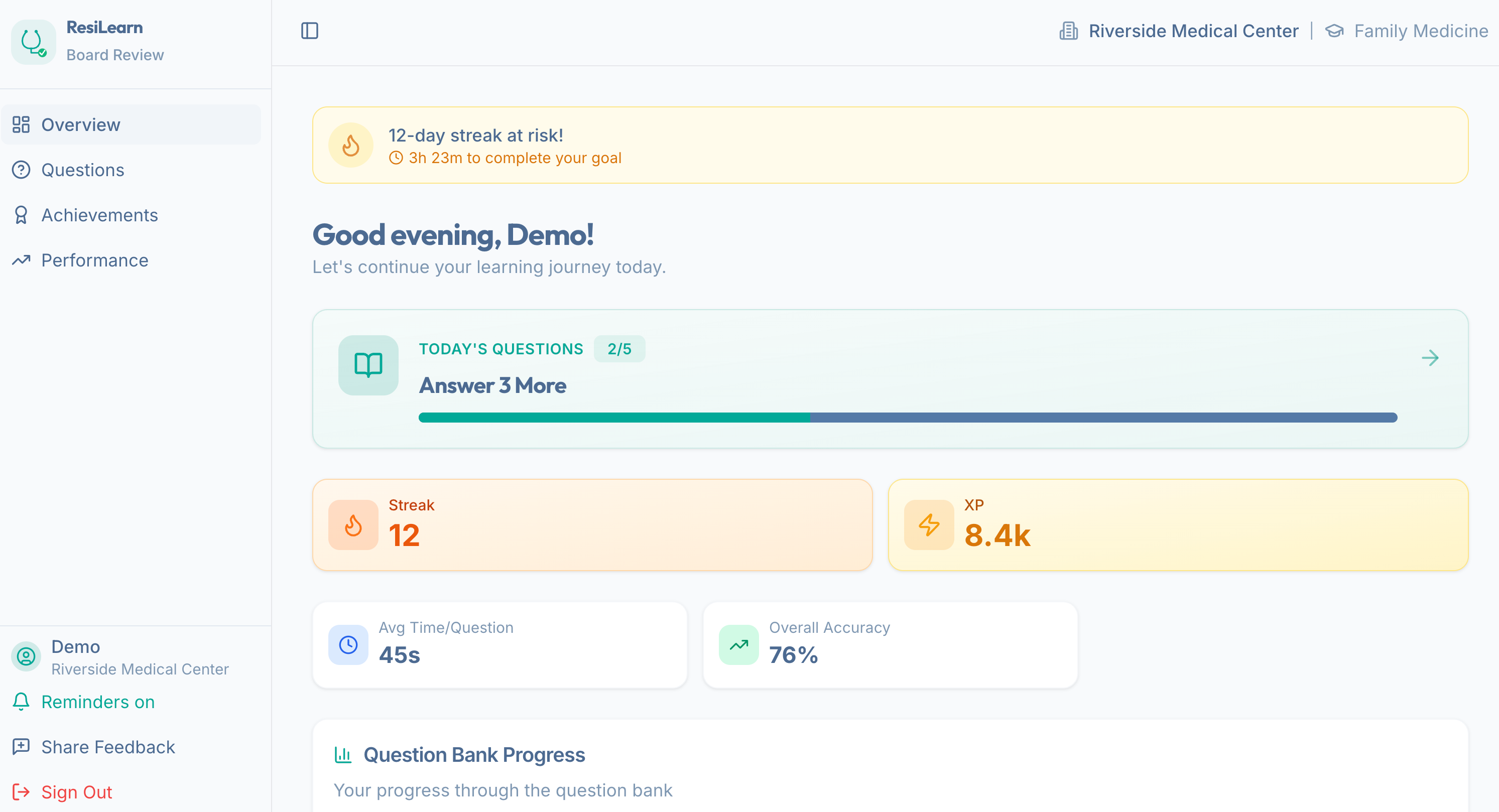
The resident-facing side of ResiLearn is built around a premise: traditional studying is boring and disconnected from how human motivation actually works. So I borrowed from the science of engagement — I studied why people can’t stop using certain mobile games, Peleton, Strava, SnapChat, and applied it to board prep.
Streaks keep residents coming back daily (the same psychology that has you opening Duolingo at 11pm even though you’ve been saying “I’ll learn Spanish someday” for years)
XP and Leaderboards tap into the healthy competition — so we channel that energy
Adaptive Learning identifies personal weak spots and serves targeted questions — so instead of reviewing cardiology for the fourteenth time, you’re actually working on what you need
Then (hoped for) result: daily engagement. Residents who study a little every day instead of a lot the week before a high-stakes exam.
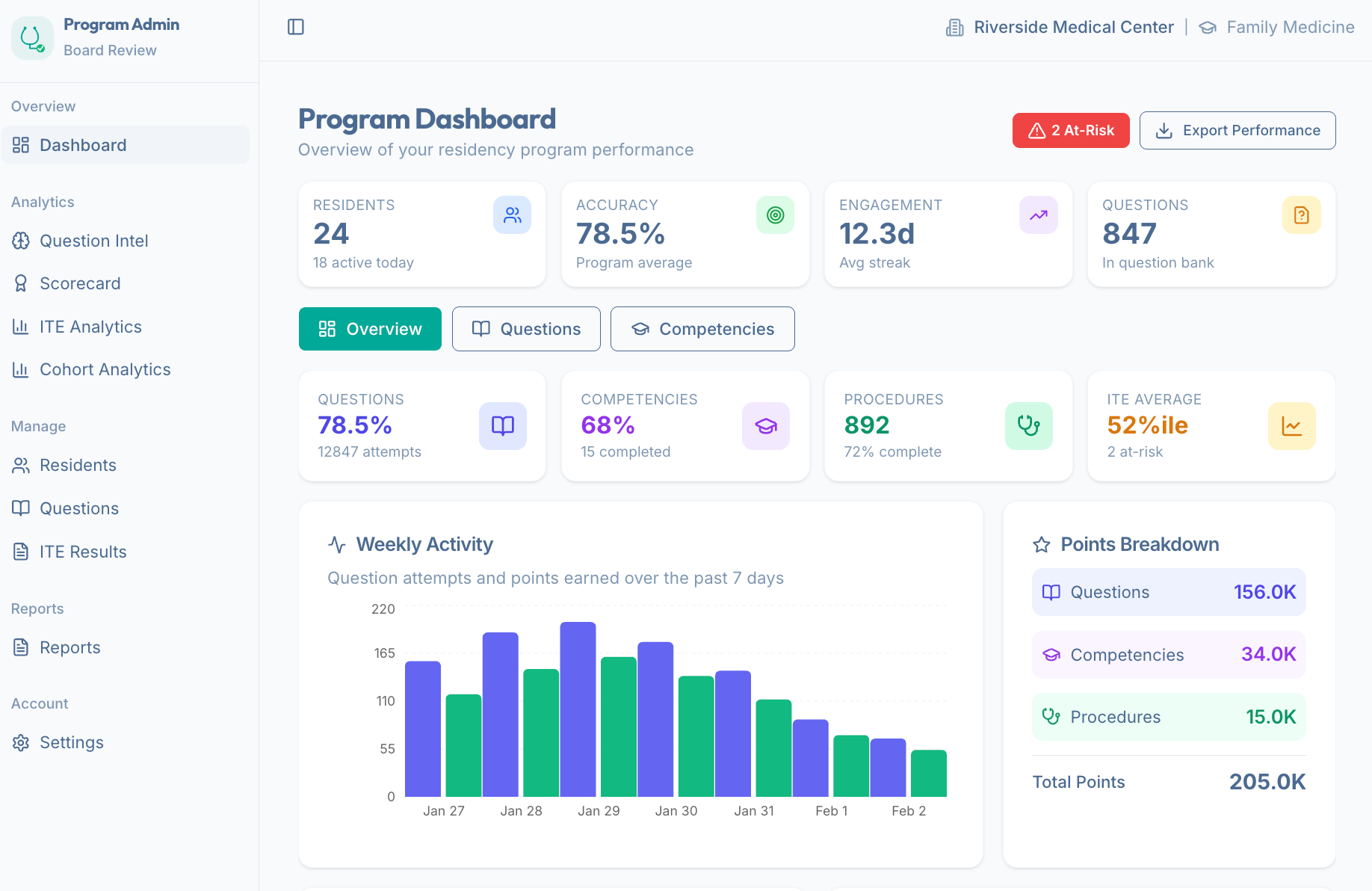
📊 For Program Directors: Stop Guessing. Start Knowing.
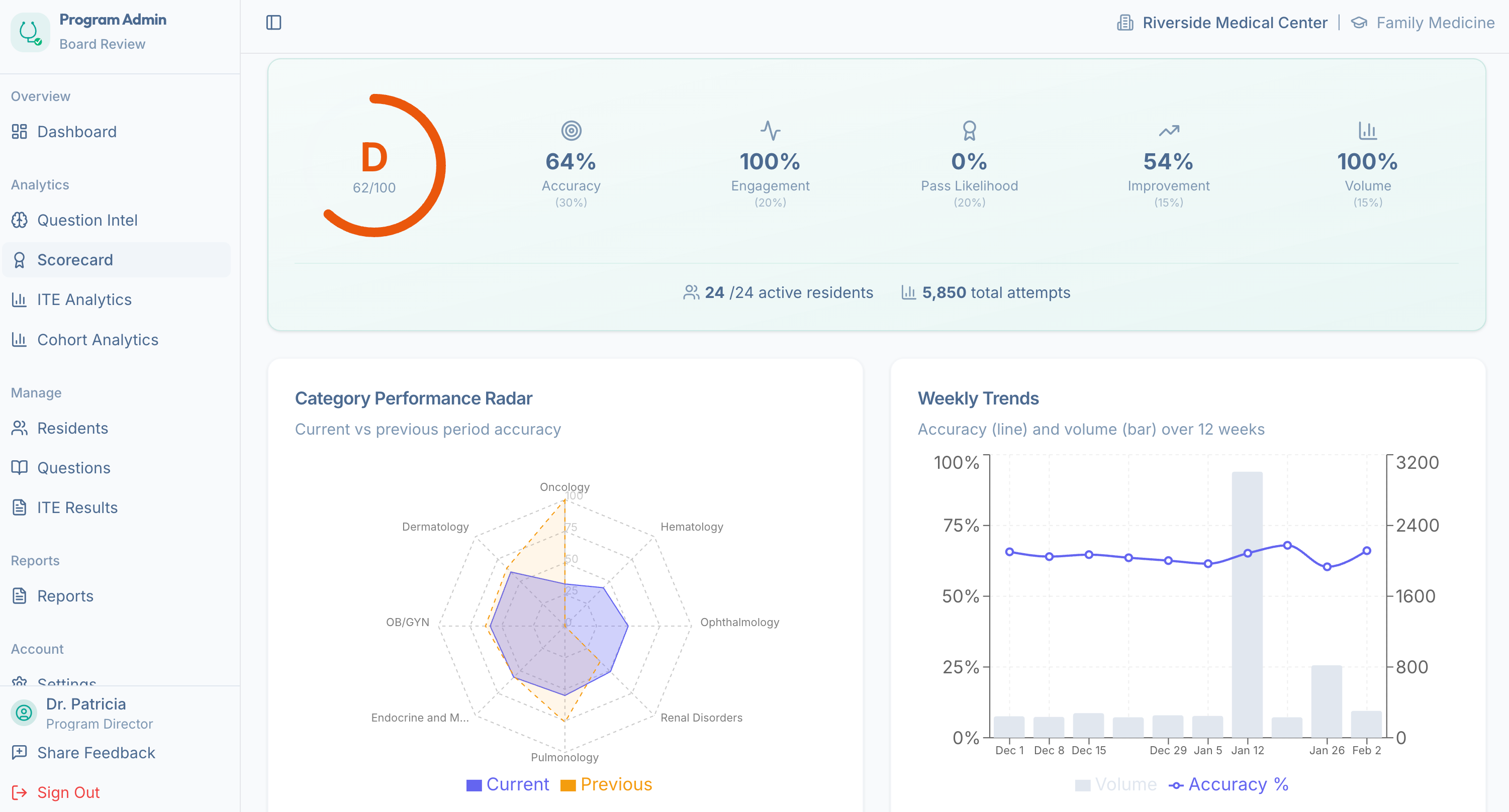
The program director side is where I poured the most of the effort.
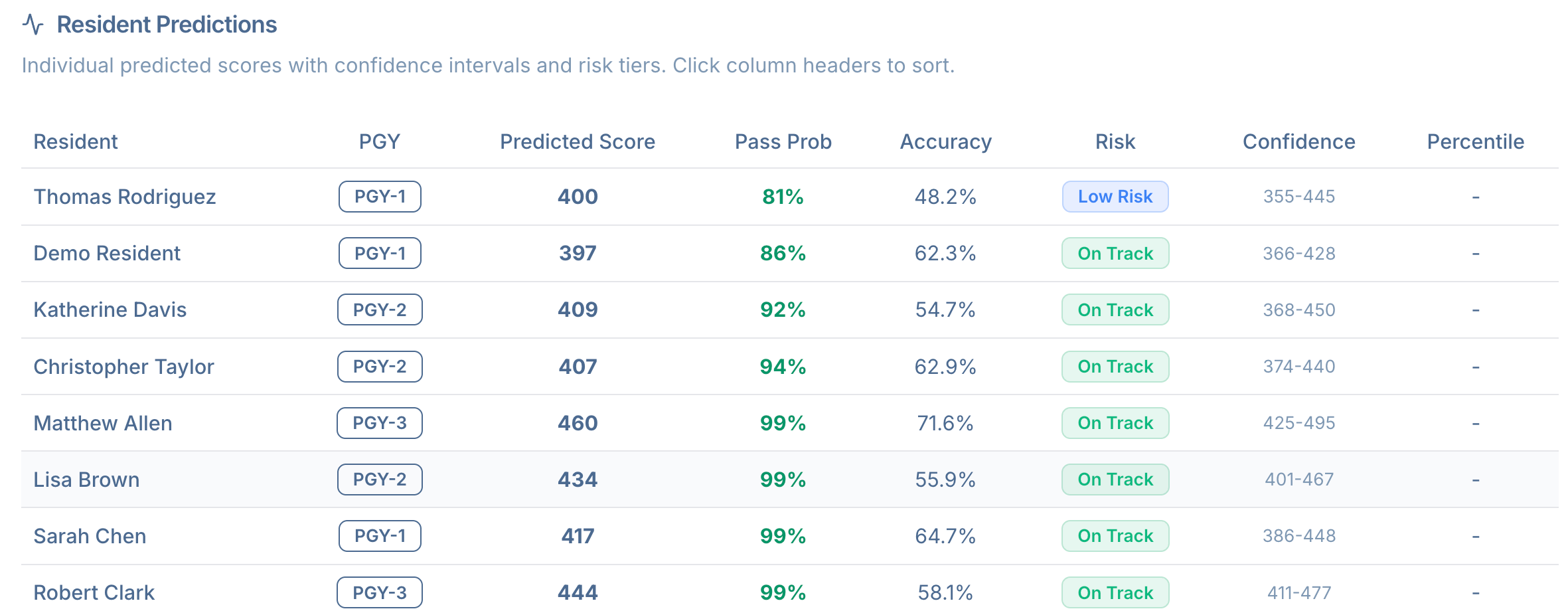
The dashboard gives you a real-time view of every resident’s performance — not a once-a-year snapshot. It includes:
Automated At-Risk Alerts that flag struggling residents before the ITE, so you can intervene instead of react
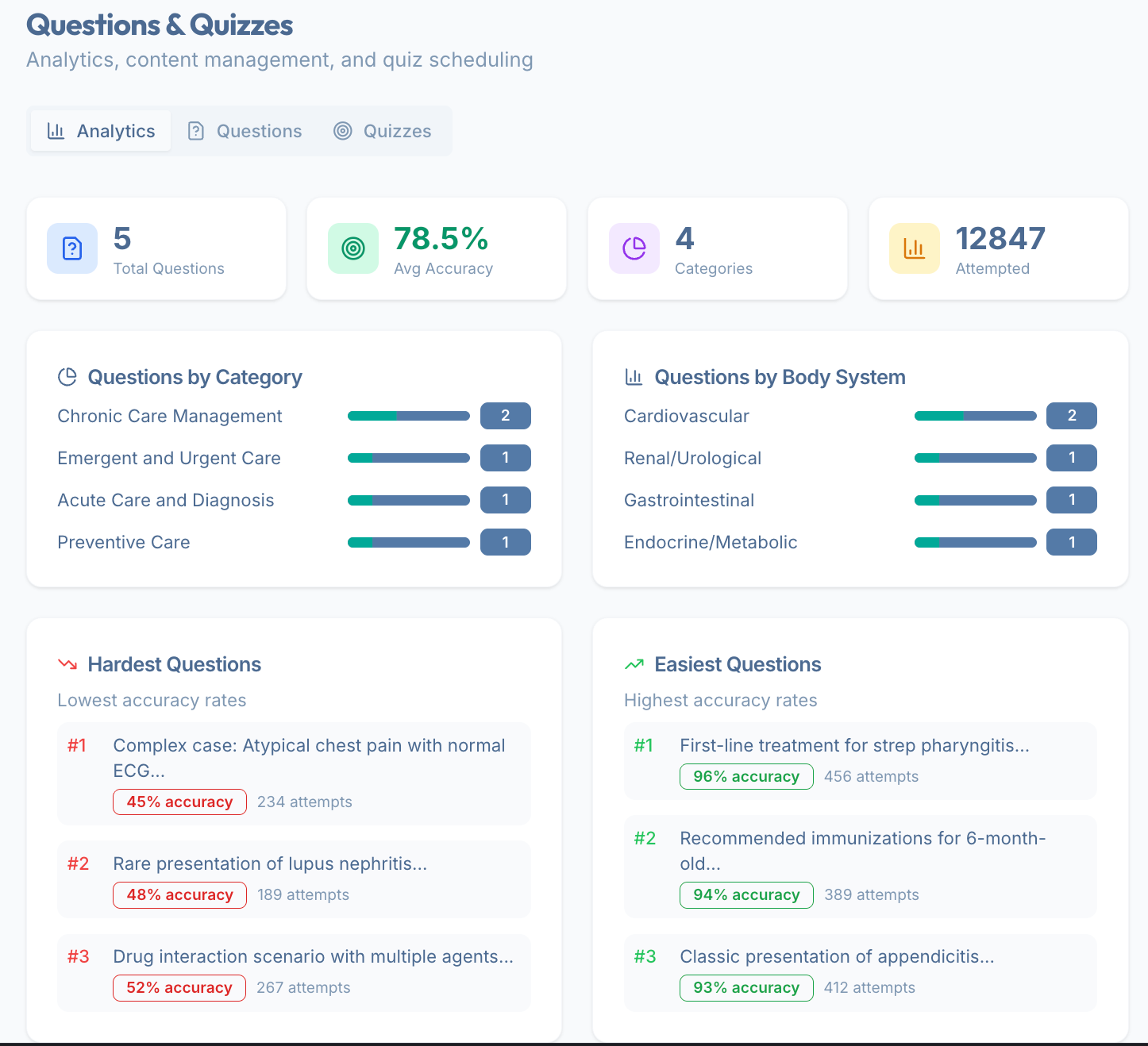
Competency Gap Analysis showing exactly which topic areas your cohort is weak in — Cardiology, Nephrology, Behavioral Health, you name it
ITE Score Predictions using their real scores, with the Bayesian predictor, performance trends to forecast outcomes and guide resource allocation
No more being blindsided.
🎯 Goal Setting That Actually Matches Real Life
A resident on a tough inpatient medicine month cannot realistically hit the same daily study targets as a resident on a lighter ambulatory week. ResiLearn lets program directors configure rotation-specific expectations.
The Science
Spaced Repetition — questions served at optimized intervals for long-term retention, not just short-term cramming.
Self-Determination Theory — the platform is designed to satisfy the three core psychological needs that drive intrinsic motivation: autonomy, competence, and relatedness.
Gamification — studies show gamification can increase engagement by up to 48% and improve learning outcomes by 34% in higher education settings.
Who Is This For Right Now?
ResiLearn is currently being built for Family Medicine residency programs only.
This is (hopefully) not forever. But right now, as we build, validate, and refine, I want to start close to the world I know best and before we expand. So please be patient.
Want to Join the Pilot?
We are actively recruiting programs for our formal pilot cohort study. If you’re a Family Medicine program director who is tired of surprises, and ready to give your residents a more sustainable path to success — I want to hear from you.
👉 Fill out our pilot interest survey
Why I’m Sharing This Here
I started this newsletter to think out loud about AI in medical education. ResiLearn is what happens when those thoughts collide with a genuine problem, and a few late nights.
I share this because the story matters beyond ResiLearn itself. The barriers between “I see a problem” and “I built something to fix it” are addressable. Every educator reading this newsletter who has spotted a gap and thought someone should fix that — that someone might actually be you.
Check out ResiLearn.com and test the demo!
💌 As always, thanks for reading. Get in touch and let me know your thoughts!
Thank you for joining us on this adventure. Stay tuned for more AI insights, best practices, and more future editions of AI+MedEd.
For education and innovation,
Karim
Share this with someone - have them sign up here.